Health officials in the Democratic Republic of the Congo(WHO) have hailed the recovery of five Ebola patients, offering a much-needed glimmer of hope even as a rapidly expanding outbreak of the rare Bundibugyo strain stretches regional health systems.
The World Health Organization (WHO) has warmly welcomed the recoveries, which involve a rare strain of the virus for which there is currently no approved vaccine or specific treatment. The news provides a vital morale boost for frontline medical teams battling an intensifying situation.
WHO Director-General Dr. Tedros Adhanom Ghebreyesus announced the milestone on Sunday during a visit to a newly opened Ebola treatment centre in the eastern Congolese city of Bunia, the capital of Ituri province.
“Four people will be discharged today, and there was one that was discharged the day before yesterday,” Dr. Tedros said, marking a rare moment of celebration in what has already become a severe health crisis.
A rapidly escalating crisis
Despite the positive news from the treatment ward, the wider epidemic, the 17th Ebola outbreak to hit the DRC—is expanding swiftly. Declared just two weeks ago, the outbreak has already claimed the lives of more than 220 people from suspected cases.
According to the latest WHO figures, the situation has intensified significantly over the past week. Health officials have tracked more than 900 suspected cases in the DRC alone. Across both nations, confirmed cases have jumped to 134, an increase of nearly 50 infections in just a matter of days.
The outbreak has also touched the international medical community. An American doctor who contracted the virus while treating patients in the DRC has been medically evacuated and is currently receiving specialist care in Germany.
Violence and logistics hamper containment
The epicenter remains firmly gripped by crisis in the DRC’s conflict-torn northeastern provinces, particularly Ituri, which accounts for nearly 90% of all confirmed cases. Managing an epidemic in this region is notoriously difficult, and the WHO warns that healthcare workers are facing a dual threat of deep-seated community mistrust and direct violence.
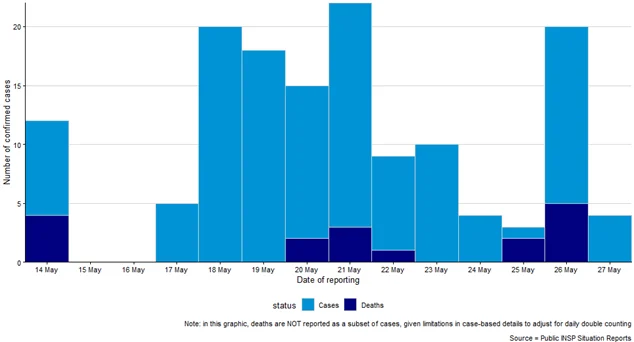
Number-of-confirmed-cases-in DRC Source Ministry of Health DRC
Recent attacks on health facilities in the towns of Mongbwalu and Rwampara have severely disrupted containment efforts. When medical teams cannot safely enter communities, contact tracing breaks down, leaving the virus to spread undetected.
Testing capacity is also under immense strain. While hundreds of samples have been processed, a backlog of more than 100 tests has been flown to the capital, Kinshasa, meaning the current official toll of 17 confirmed deaths in the DRC is almost certainly an underestimate. Crucially, 16 health workers are among those who have tested positive, underscoring the extreme risks faced by frontline staff.
Cross-border spread to Uganda
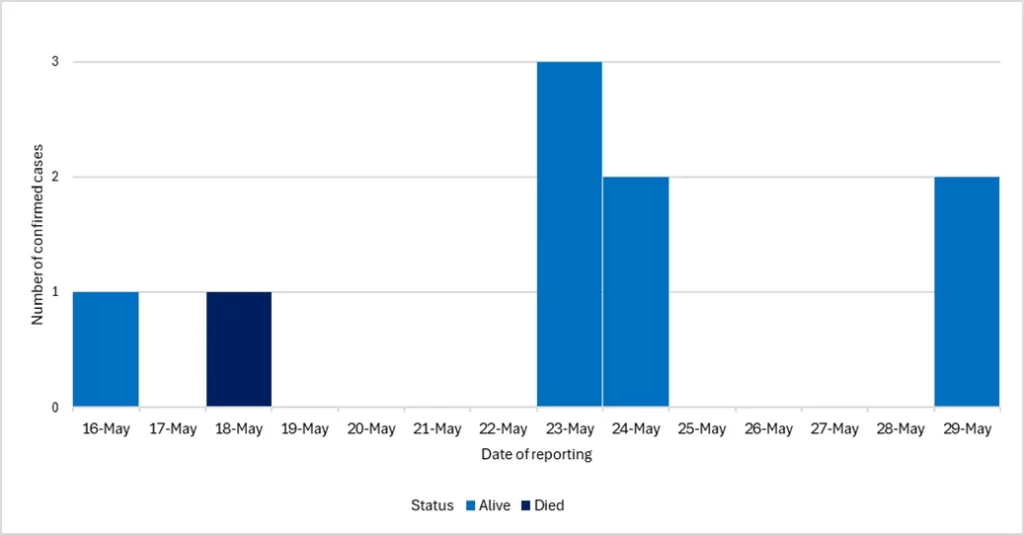
Meanwhile, Uganda is racing to contain its own cluster of cases, centered primarily around Kampala and neighboring Wakiso. Nine cases have been confirmed there so far, including one death.
Number of confirmed cases and deaths by date of reporting in Uganda as of 29 May 2026 Source Ministry of Health Uganda
The virus traveled across the porous border via routine local transit. Those currently under monitoring include a Ugandan driver who transported an early patient, and a Congolese woman who had crossed the border seeking medical treatment. Roughly 436 people in Uganda are now being monitored to prevent the virus from taking a firmer hold in the capital.
What is the Bundibugyo strain?
While the word “Ebola” often brings to mind the highly lethal Zaire strain that caused the devastating West African epidemic a decade ago, the Bundibugyo virus (BVD) is a distinct species within the Orthoebolavirus family.
The Challenge of Bundibugyo:
Unlike more common strains of Ebola, there are currently no approved vaccines or specific antiviral treatments for the Bundibugyo virus.
Historically, it has a slightly lower case fatality rate than the Zaire strain, hovering between 30% and 50% in previous outbreaks, but it remains an incredibly dangerous pathogen.
Because early symptoms are entirely non-specific, fever, headaches, muscle aches, and a sore throat, it is frequently mistaken for malaria or typhoid. By the time severe gastrointestinal symptoms or bleeding begin, the virus has often already spread to family members or hospital staff. This is why the survival and discharge of these five patients is being watched so closely.
The Global Response
The escalating crisis prompted the emergency visit to the DRC by Dr. Tedros to review frontline operations firsthand and open the new isolation facilities in Bunia.
The WHO currently assesses the risk as “very high” at the national level for the DRC and “high” regionally, though the threat to the wider world remains low. Despite the high regional risk, international health officials are advising against any restrictions on travel or trade, warning that border closures often backfire by driving trade underground and crippling local economies.
Instead, the strategy relies entirely on the hard-won fundamentals of outbreak control: keeping healthcare workers safe, building community trust, and tracking down every single individual who may have been exposed.















{kind=link}